- Original Article
- Open access
- Published:
Daflon use for reducing post-tonsillectomy pain and hemorrhage: a prospective study
The Egyptian Journal of Otolaryngology volume 37, Article number: 20 (2021)
Abstract
Background
Tonsillectomy usually was a safe procedure; in adults, the risk of agonizing pain and secondary hemorrhage could be serious. We introduced Daflon as a safe and effective complementary medication in reducing these risks. This prospective study was designed to evaluate the effect of using (Daflon oral medication) on post-tonsillectomy pain and hemorrhage rates. This study was conducted on 60 patients of both sexes, above 21 years, and underwent tonsillectomy using bipolar diathermy. Patients were randomly distributed between 2 groups; each group has 30 patients and with the same post-operative protocol; in group 2, an addition of Daflon 500 mg tablet twice daily for 14 days post-operatively was given.
Results
In group 2, agonizing pain start day, pain duration, analgesia duration, and need for another type, all were significantly different from group 1, starting day in group 1 (4.3 ± 4.0) and (7.2 ± 1.3) in group 2, pain duration in group 1 (7.3 ± 1.5) and (4.2 ± 1.4) in group 2 and need for more analgesia 80% in group 1 and 50% in group 2. Post-operative hemorrhage was 4 cases (13.3%) in group 1, and 2 cases (7%) in group 2, also severity of post-operative bleeding were less in group 2. Healing membrane detaching time was (12.2 ± 2.2) in group 1 and (9.1 ± 1.9) in group 2.
Conclusion
The use of Daflon 500 mg tablet after bipolar tonsillectomy added to effectiveness of pain control also could help in reducing bleeding rates and its severity. Overall, its use enhances recovery and improves quality of life.
Background
Tonsillectomy is one of the oldest and most common procedures done in ENT specialty over the years. The spectrum for indication of this procedure is so variable and still surgeon dependant, although many guide lines were introduced. Two major categories of indications: first, infective causes (recurrent, chronic-tonsillitis, quinsy) which represents the majority indications. Second, the non-infective causes including snoring, apnea, halitosis, biopsy, etc. consists for the other part [1,2,3].
Pain and bleeding (either primary or secondary) stay the most common annoying and serious post-operative complications [4].
Intense pain is one of the most important post-operative complaints, and in 20% of cases, it represents one of the common causes for hospital revisit, dehydration, and possibly re-admission [5].
Many researches correlate pain intensity with the surgical technique (less with cold steel and more severe in diathermy or laser tonsillectomies). Chronic tonsillitis with fibrosis in bed (more dissection) is associated with more rates of postoperative pain. Increasing age, adults were found to experience more postoperative pain which is logic and may be referred to less healing power, more infection, and wider healing surgical bed [6, 7].
Different modalities of perioperative and postoperative medical protocols were tried in hope to reduce post-tonsillectomy pain. Perioperative antimicrobial steroids were proved effective in reducing postoperative pain and subsequent complications. Good analgesia and hydration is still one of the basic postoperative protocols [8].
Bleeding after tonsillectomy is still one of the most distressing complications for both patients and doctors. Like post-tonsillectomy pain, it was related to patient age (increasing rates of bleeding in adults), sepsis, chronicity, and anemia also have high rates of bleeding. Lastly, the adequate post-operative analgesia and hydration helps to reduce bleeding rates [9].
Multiple published rates for primary and reactive post-tonsillectomy hemorrhage vary from 0.3 to 2.1%, while those for secondary bleeding ranged from 2 to 20% [10].
Many papers evaluated the correlation between technique used and the incidence of post-tonsillectomy hemorrhage. Most of results were so variable and even contradictory, but the main consensus that bipolar diathermy tonsillectomy as safe and effective procedure is still valid (Table 1) [11].
In 1971, Daflon (90% Diosimin and 10% Hesperidin) was first introduced in France by Bensuade et al. for treatments of various capillovenous disorders [12].
It works through stabilizing vascular wall, increasing its integrity and contractility with protection of vascular endothelium. Daflon has also anti-inflammatory effect through decreasing the synthesis of prostaglandins (PGE2 and thromboxane B2), reduction of leukotriene and other mediators. This effects decreases edema, local pain, and prompts healing [13].
Since that time, it was used safely in variant indications, ages, even in pregnancy, still its use in ENT is very limited (mostly in Epistaxis), recent papers started to investigate its vascular and anti-inflammatory properties in other indications as vasomotor rhinitis of pregnancy. Based on this and more, we had the idea and courage to start this research [14].
Aim of work
This work was designed as a prospective randomized study to evaluate the effect of using Daflon on reducing post-tonsillectomy pain and hemorrhage.
Methods
This prospective study was designed to include 60 adult patients of both sexes undergoing adult bipolar dissection tonsillectomy during the period between October 2016 and October 2018. All patients were above 21 years, approved to join the study, and signed a clear informed consent, after complete information about protocol, benefits, and risks. The study was approved by the hospital medical ethical committee (Dallah Hospital KSA 2016).
All patients fulfilling the selection criteria were randomly distributed between the two groups. Group 1 (included 30 patients) underwent the standard surgical and post-operative protocol, and in group 2 (30 patients), the same protocol was conducted in addition to Daflon 500 tablets 12 hourly, for 14 days post-operatively.
Age of patients was between 21 and 45 years, and they were free from chronic systemic disorders (DM, HTN, CVS, renal, liver). Tonsillectomy indications were limited to chronic tonsillitis; snoring and apnea procedures only.
Concurrent adenoidectomy or myringotomy with tube insertion, acute infection, previous quinsy, bleeding disorder and allergy to (paracetamol, diclophenac, and amoxicillin-clavulanic acid) were excluded from the study.
All surgeries in both groups were done using bipolar diathermy (careful dissection, low energy, minimal tissue trauma as much as possible), under general anesthesia with effective pain control measures (perioperative antibiotic prophylaxis, IV steroids, analgesics, and good hydration).
The standard post-operative medical follow-up care included at least 10 days of paracetamol 1 mg 8 hourly, local antiseptic and soothing mouth wash, and systemic antibiotics (amoxicillin-clavulanic acid) 1 mg BID, all for at least 10 days and (diclophenac) on need.
We designed a special post-operative follow-up schedule for clinical examination, observation, and questionnaire about pain, dysphagia, post-operative bleeding, and healing of tonsillar bed as follows:
-
I
Pain was assessed through:
-
1.
Pain intensity scoring (0–10 according to visual analogue scale) (Fig. 1) [15].
-
2.
Agonizing pain duration (number of days where more analgesia needed/severe dysphagia).
-
3.
Need for additional dose of paracetamol or additional other type (yes/no). Diclophenac 150 mg maximum dose divided BID OR TID.
-
4.
Duration of swallowing difficulties (number of days of dysphagia).
-
5.
Degree of dysphagia: [16].
-
0
= no dysphagia
-
1
= mild discomfort during swallowing solid foods, but fluids pass freely.
-
2
= moderate discomfort during swallowing solid foods, and fluids.
-
3
= severe discomfort during swallowing solid foods, and fluids.
-
4
= serious difficulties in both eating and fluids swallowing, or, no swallowing.
Fig. 1 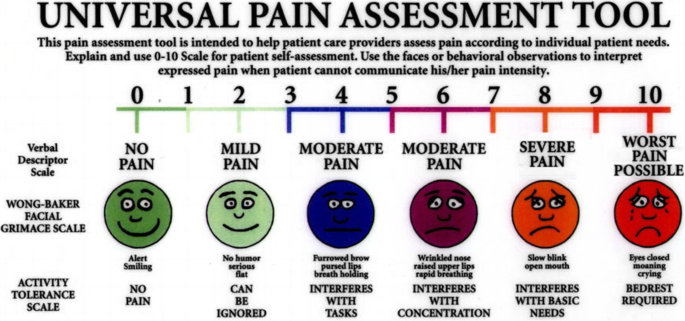
Universal visual analog scale for pain assessment [15]

-
II
Post-tonsillectomy bleeding:
-
1.
Day of bleeding occurrence.
-
2.
Grading of bleeding episode: [17]
Grade A: blood-tinged sputum.
-
(a)
A1: Wound is and stays dry, no coagulum upon inspection.
-
(b)
A2: Coagulum upon inspection, dry wound after removal.
Grade B: Bleeding actively under examination, medical treatment was necessary, dry wound afterwards, blood count in normal range, no shock.
Grade C: Surgical treatment with general anesthesia was needed to stop bleeding, blood count still in normal range, no shock.
Grade D: Dramatic hemorrhage, hemoglobin decreased, blood transfusion required advanced surgical treatment, intensive care may be necessary.
-
3.
Risk factors (severe pain, no swallowing, secondary infection, and fever).
III-Healing membrane detaching time and degree of body weight loss at 10th day (fasting body weight at day of surgery–fasting body weight at day 10) will be used as parameters for scoring good recovery and good health.
-
III
Healing membrane detaching time and degree of body weight loss at 10th day (fasting body weight at day of surgery–fasting body weight at day 10) will be used as parameters for scoring good recovery and good health.
Statistical analysis
Statistical analyses of the collected data were done by using SPSS version 17. Quantitative data were presented as mean and standard deviation and were analyzed by using one-way ANOVA test. Qualitative data was presented as numbers and percentages and were analyzed by using chi-square test and fisher extract test. P value < 0.05 was considered significant white P value < 0.01 was considered highly significant.
Results
This study was conducted on 60 adult patients operated for tonsillectomy. Age was ranging from 21 to 45 years, with mean ± SD of 28.88 ± 10.2 in group 1 and 29.31 ± 12.1 in group 2 with no significant difference between the two groups.
Sex distribution in this study was 33 males (55%) and 27 females (45%) with no significant difference between the two groups.
With regard to pain, group 1 showed early pain starting day (4.3), longer duration (7.3) and more need for analgesia (80%) either adding diclophenac or extending the duration (7 days), on the other hand, group 2 showed significant contradictory differences in all aspects (7.2, 4.2, 50%, 5.2, respectively) (Table 2).
There was statistically significant difference between the two groups with respect to pain intensity score post-operatively according (universal pain assessment visual analogue scoring system from 0 to 10) that reported in 5th, 10th, and 15th day with score in favor of group 2 (Table 3).
Dysphagia duration per day post-operatively was significantly higher among patients of group 1 (Table 4).
Group 2 with Daflon added showed statistically significant less dysphagia scoring that reported in 5th, 10th, and 15th day (Table 5).
Post-tonsillectomy secondary hemorrhage was reported in 4 cases in group 1, and 4 cases in group 2, with no significant statistical differences (Table 6).
According to the severity of post-tonsillectomy hemorrhage that range from blood-tinged sputum up to dramatic hemorrhage which need blood transfusion and surgical intervention ± intensive care admission, we had no significant difference among patients of both groups, although the distribution was in favor of group 2 regarding less severity of bleeding (Table 7).
Bleeding risk factors showed no significant differences between both groups. (Table 8).
The time of detaching of healing membrane as an indicator of healing was found significantly good and early in group 2 (Table 9).
Body weight loss on an empty stomach on the 10th day post-operatively as a good sign of recovery was significantly better and less body weight loss in group 2 (Table 10).
Discussion
Tonsillectomy is among the oldest and most commonly performed procedures in the field of otolaryngology. Approximately 530,000 outpatient adeno-tonsillectomies were performed annually in US hospitals [18].
Post-operative complications are almost rare, but pain and secondary hemorrhage are considered the most serious and could be life threatening events [19].
Our results were independent on demographic variable. All operations were performed by the same surgeons with the same technique. Strict inclusion and exclusion criteria were applied to ensure standardization of most variables and to prevent the introduction of confounding factors.
Although the study was randomized, there was no statistically significant difference between two groups regarding age and sex, and this adds to the consistency of the results.
The main aim of the study was to test effectiveness of Daflon use on post-operative pain reduction; we found strong significant pain reduction in group 2 in all parameters tested. Agonizing pain start day was late in group 2 and it was near the 7th day; in group 1, it was near 4th day which was previously agreed by Zagolski et al. who proved that pain scores after dissection tonsillectomy, as measured by visual analog scale, differed significantly between every third consecutive days following post-operative day 4. Two-thirds of the patients required analgesics after the first post-operative day [16].
Also, agonizing pain duration was reduced significantly to about 4 days in group 2 in comparison to 7 days in group 1, with subsequent reduction in analgesia doses and need to add diclophenac. Total pain duration in group 2 was near to 6 days, and in group 2, it was near to 10; these numbers regarding group 1 was consistent with literature which demonstrated pain duration from 10 to 14 days post-operatively, and they stated that about 80% of the individuals returned to work within 14 days of surgery and almost all reported normal swallowing within 14 days of surgery. The worst pain level in group 1 was 7 by (VAS), and in group 2 was 5, which was comparable to results of Arbin et al. which demonstrated scores of pain of 6.9 with bipolar tonsillectomy [20].
We used dysphagia as another indicator for pain intensity and duration, as it was more objective and added to more consistency of our results. Zagolski et al. stated dysphagia duration near 11 days in contrast to our study, and we had reported approximately 7 days in group 1 and 5 in group 2; these results were highly statistically significant in favor of Daflon use in group 2 [16].
Dysphagia duration still a crude test with multiple grades and multiple variants inside, so we used the objective dysphagia grading system for correlating post-operative parameters and return to normal life. In our study, the time interval from 5th day to 10th day was found the maximum pain and dysphagia period; the score was significantly high in group 1 and has longer duration [21].
In literature, there was a great difference in the reported incidence rates of post-tonsillectomy hemorrhage, ranging between 0.28% and 20%, and the older age of patient was consistently been described a major risk factor for bleeding [22]. Here, in this study, we had secondary post-tonsillectomy hemorrhage rates 13.3% in group 1, and 7% in group 2 which matched other reviews. We did not depend on primary and reactionary hemorrhage rates as it were strongly related to patient preoperative preparation and technical operative defects [10].
Post-tonsillectomy hemorrhage grading starts from blood-tinged sputum to dramatic hemorrhage; we used the highly practical scale provided by Sarny et al. 2011 [17]. Although there was no significant difference between the two groups, but the grading severity comes in favor with group 2, this statistical result could be attributed to narrow sample size. In group 2, we had no case of post-tonsillectomy secondary hemorrhage in grade D, C, or B; the two cases fall in the very mild grade A1 and A2 which entailed only conservative medical management. In contrast to group 2 where the four cases ranged from grade A to C in which surgical control was applied. The risk factors predisposing for secondary bleeding were analyzed in both groups, with no significant difference appeared in all parameters which added to consistency of the study.
We had chosen healing membrane detaching time and degree of body weight loss at 10th day as two objective parameters for degree of sense of wellness, return to normal life, and of course indicating effective healing. These parameters and others were tested effectively in the study of Salonen et al. 2004 and Zagolski et al. 2016 [4, 16].
Healing membrane detachment time was significantly earlier by 2–3 days in group and weight loss also was significantly low by about 2 kg in the same group. This was better than the results reported by Zagolski et al in 2015 that range from 4.6 to 5.4 kg [23].
Since 1971, Daflon was used safely and effectively in treating different kinds of vascular disorders, in general surgery, vascular, and obstetric specialties. Previously used as effective treatment in vasomotor rhinitis of pregnancy in ENT, now we introduce it as adjunctive treatment in post-tonsillectomy adult patients, making use of its healing and anti-inflammatory properties in decreasing post-operative pain, dysphagia, and secondary bleeding [14].
The strengths of this study came from direct comparison of statistically significant groups operated for the same symptoms using the same technique and trying as much as possible to avoid any bias in inclusion and exclusion criteria. Small sample size was the weakness point, but this is a novel study not done before need to be tested on wide scale and in multicenter studies
Conclusion
In adult tonsillectomy, we could introduce Daflon as an effective adjunctive medication that significantly reduced pain, dysphagia, accelerated healing, and rapid recovery. Also, it could possibly reduce the rate and severity of secondary post-tonsillectomy hemorrhage.
Availability of data and materials
I/we certify that all the data collected during the study is presented in this manuscript and no data from the study has been or will be published separately. We attest that, if requested by the editors, we will provide the data/information or will cooperate fully in obtaining and providing the data/information on which the manuscript is based, for examination by the editors or their assignees.
References
Negm A, Atef A, Lasheen H, Kamel A, Azooz K, Elhoussainy O (2017) Factors affecting secondary post-tonsillectomy hemorrhage: a case control study. Egypt J Otolaryngol 33(1):50–55
Silva S, Ouda M, Mathanakumara S, Ridyard E, Morar P (2012) Tonsillectomy under threat: auditing the indications for performing tonsillectomy. J Laryngol Otol 126:609–611
Hoddeson EK, Gourin CG (2009) Adult tonsillectomy: current indications and outcomes. Otolaryngol Head Neck Surg 140:19–22
Salonen A, Kokki H, Nuutinen J (2002) Recovery after tonsillectomy in adults: a three-week follow-up study. Laryngoscope. 112:94–98
Ragab SM (2012) Six years of evidence-based adult dissection tonsillectomy with ultrasonic scalpel, bipolar electrocautery, bipolar radiofrequency or ‘cold steel’ dissection. J Laryngol Otol 126:1056–1062
Hiller A, Silvanto M, Savolainen S, Tarkkila P (2004) Propacetamol and diclofenac alone and in combination for analgesia after elective tonsillectomy. Acta Anaesthesiol Scand 48:1185–1189
Sarny S, Habermann W, Ossimitz G, Stammberger H (2012) Significant post-tonsillectomy pain is associated with increased risk of hemorrhage. Ann Otol Rhinol Laryngol 121:776–781
Murthy P, Laing MR (1998) Dissection tonsillectomy: pattern of postoperative pain, medication and resumption of normal activity. J Laryngol Otol 112:41–44
Lee MSW, Montague ML, Musheer Hussain SS (2004) Post-tonsillectomy hemorrhage: cold versus hot dissection. Otolaryngol Head Neck Surg 131:833–836
Liu J, Anderson K, Williging J, et al. Post-tonsillectomy Hemorrhage. Arch Otolaryngol Head Neck Surg. 127:1271-75.
Walker P, Gillies D (2007) Post-tonsillectomy hemorrhage rates: Are they technique-dependant? Otolaryngol Head Neck Surg 136:S 27–S 31
Bensaude A, Vignle R, Naouri J (1972) The medical treatment of acute haemorrhoidal premenstrual episodes and haemorrhoidal congestion. La Vie Medicate 1971 S2:39–45
La torre F, Nicolai AP (2004) Clinical use of micronizaed purified flavonoid fraction for treatment of symptoms after haemorrhoidectomy: results of a randomized, controlled, clinical trial. Dis Colon Rectum 47:704–710
Ezzat W, Fawaz S, Makhazangy A, Rateb A (2009) Role of Diosmin-Hesperidin combination (Daflon) in treatment of vasomotor rhinitis of pregnancy; Randomized control study. Egypt J. Otolaryngol 25(1):61–65
Jones DT, Yoon MJ, Licameli G (2007) Effectiveness of postoperative follow-up telephone interviews for patients who underwentadenotonsillectomy: a retrospective study. Arch OtolaryngolHead Neck Surg 133:1091–1095
Zagólski O, Gajda M, Strek P, Kozlowski M, Gadek A, Nyzio J (2016) Adult tonsillectomy: postoperative pain depends on indications!! Braz. J Otorhinolaryngol 82(5):589–595
Sarny S, Habermann W, Ossimitz G, Schmid C, Stammberger H (2011) Tonsillar haemorrhage and re-admission: a questionnaire based study. Eur Arch Otorhinolaryngol 268:1803–1807
Cullen KA, Hall MJ, Golosinskiy A National Health Statistics Reports. Number 11. 2006. Centers for disease control. Ambulatory Surgery in the United States
Windfuhr JP, Chen YS, Remmert S (2005) Hemorrhage following tonsillectomy and adenoidectomy in 15,218 patients. Otolaryngol Head Neck Surg 132:281–286
Arbin L, Enlund M, Knuttsson J (2017) Post-tonsillectomy pain after using bipolar diathermy scissors or the harmonic scalpel: a randomized blinded study. Eur Arch Otorhinolaryngol 017:4451–4459
Pizzuto MP, Brodsky L, Duffy L et al (2000) A comparison of microbipolar cautery dissection to hot knife cautery tonsillectomy. Int J Pediatr Otorhinolaryngol 52(3):239–246
Tomkinson A, Harrison W, Owens D et al (2011) Factors for postoperative hemorrhage following tonsillectomy. Laryngoscope 121:279–288
Zagólski O, Kulisiewicz J (2012) Perioperative antibiotic in adenoidec-tomy with partial tonsillectomy: a randomized trial. ORL J Otorhinolaryngol Relat Spec 74:86–92
Acknowledgements
Great thanks for Dr Salah Ramadan Ass. Prof. Cairo University, for his help and effort in data analysis and statistics interpretation, he was so helpful and cooperative.
Funding
None
Author information
Authors and Affiliations
Contributions
HR and AS authors were equally share in idea verification, pilot study preparation and conducting, study design, submitted to ethical committee, ethical approval, collecting background data, doing surgeries, post-operative follow up, out coming statistical assessment, paper writing. AS was responsible for submitting in this respected journal. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the hospital medical ethical committee (Dallah Hospital KSA 2016). All patients were above 21 years, approved to join the study, and signed a clear informed consent, after complete information about protocol, benefits, and risks
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests of any kind.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Saleh, A.S.E.S., Rabie, H.M.K. Daflon use for reducing post-tonsillectomy pain and hemorrhage: a prospective study. Egypt J Otolaryngol 37, 20 (2021). https://doi.org/10.1186/s43163-020-00060-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43163-020-00060-y